Open Nav

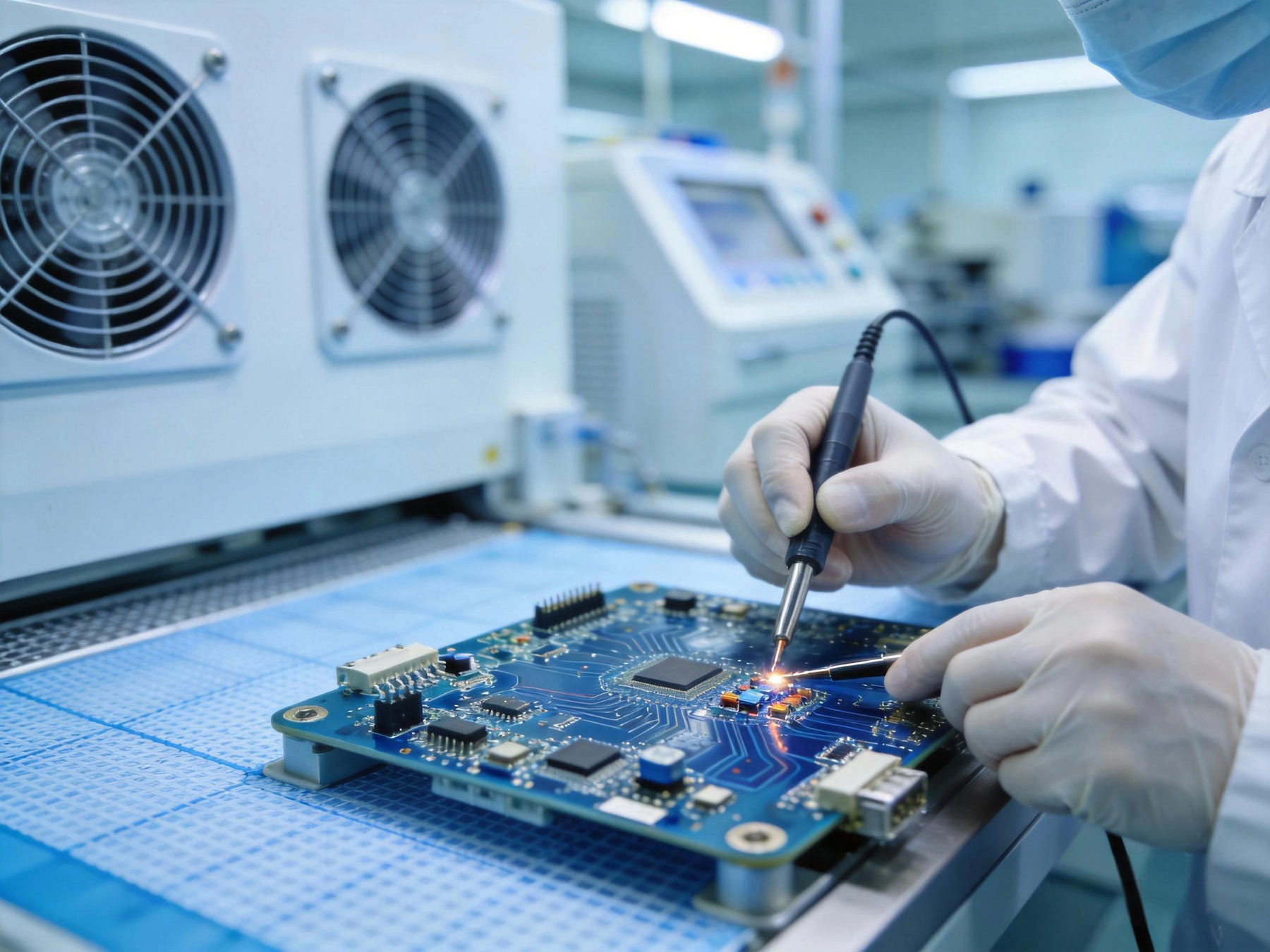
In 2019, a major infusion pump manufacturer issued a worldwide recall affecting over 700,000 units. The root cause: a solder joint failure on a Pcb that controlled drug delivery dosing. No patients were harmed, because the recall happened before the failure rate hit the level that would have caused therapeutic errors. But the incident illustrates a reality that everyone in medical device Electronics Manufacturing understands: the stakes are different here. A PCB failure in a consumer gadget is an inconvenience. A PCB failure in an insulin pump, a cardiac monitor, or a surgical robot is a clinical event. That difference shapes everything about how medical-grade PCBs are designed, assembled, tested, and documented — and why the choice of Manufacturing partner matters more in healthcare electronics than almost any other industry.
The surface difference between a medical-grade PCB and an industrial or consumer PCB is the regulatory framework: medical devices must meet FDA requirements in the US, MDR requirements in Europe, and equivalent standards in every major market. The deeper difference is that regulatory compliance is a floor, not a ceiling — and meeting the standard requires engineering depth that most EMS providers simply don't have.
Medical device PCBA operates under different constraints than most Electronics Manufacturing. The environment is often harsher — devices may be sterilized, implanted, or used in operating rooms. The consequences of failure are more severe. The documentation requirements are more extensive. The testing requirements go further. And the tolerance for field failures is essentially zero, because even a single failure event involving a patient can trigger regulatory scrutiny, mandatory recalls, and liability exposure that can threaten a company's entire product line.
These aren't reasons to avoid medical electronics — they're reasons to approach medical electronics with the seriousness they deserve. The companies that do it well — the ones whose devices are trusted in hospitals and clinics worldwide — have built their Manufacturing capabilities around the principle that every process decision is ultimately a patient safety decision.
Iso 13485 is the foundational Quality Management standard for Medical Device Manufacturing. It establishes the framework for everything from design controls and supplier management to process validation and complaint handling. FDA 21 CFR Part 820 (Quality System Regulation) imposes equivalent requirements for devices sold in the US, and the EU's MDR (Medical Device Regulation) adds additional obligations on top of Iso 13485.
For Pcb Assembly specifically, ISO 13485 requires that manufacturers maintain documented processes for every step that affects product quality — from incoming component inspection through assembly, inspection, testing, and packaging. It requires validation of manufacturing processes (you have to prove that your assembly process consistently produces boards that meet specifications), control of nonconforming product, and a corrective and preventive action (CAPA) system that tracks quality issues from identification through resolution.
The practical impact for device manufacturers is substantial. When you audit an EMS provider's ISO 13485 quality system, you're looking for: documented work instructions for every assembly process, evidence of operator training and qualification, incoming inspection records for components, in-process inspection and testing records, device history records (DHRs) that prove each board was built to spec, and a CAPA system that has teeth — not just paper compliance that looks good in audits but doesn't actually drive improvement.
ISO 13485 certification is not the same as ISO 13485 compliance. A company can hold the certificate while operating in ways that don't fully meet the standard — certificates can lag actual practice, and auditors can't be everywhere. The real question is how the company actually operates day-to-day, not what their certificate says. This is why device companies audit their manufacturing partners thoroughly before qualifying them, not just requesting certificates.
Not all medical devices carry the same regulatory burden. The FDA classifies devices into three classes based on risk — Class I (lowest risk, like bandages), Class II (moderate risk, like infusion pumps), and Class III (highest risk, like implantable pacemakers). The classification determines how much validation, testing, and documentation is required. Higher-class devices require more rigorous assembly controls, more extensive process validation, and more comprehensive device history records.
General controls, typically exempt from premarket notification. Assembly requirements focus on basic quality systems and documentation. Examples: tongue depressors, handheld surgical instruments.
Special controls including performance standards and post-market surveillance. Requires design controls, process validation, and comprehensive DHRs. Examples: infusion pumps, diagnostic monitors.
Premarket approval (PMA) required. Most stringent controls: extensive design controls, clinical data, manufacturing process validation, and ongoing post-market surveillance. Examples: pacemakers, cochlear implants.
The higher the device class, the more rigorous the PCBA requirements. A manufacturer qualified for Class II assembly may not meet the requirements for Class III. Verify your EMS partner's validated capabilities before assuming they can handle your device class.
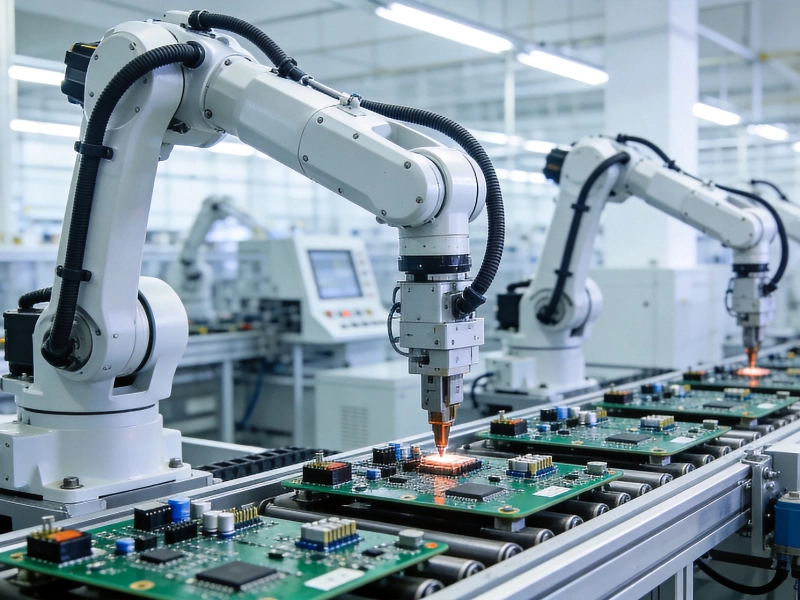
Electrostatic discharge (ESD) is one of the primary sources of latent defects in Electronics Assembly — defects that pass all inspection and functional testing and then fail in the field after months of operation. For medical devices where field failures are unacceptable, ESD control isn't optional or aspirational. It's a fundamental process requirement.
Medical device EMS facilities maintain ESD Control Programs compliant with ANSI/ESD S20.20 or equivalent standards. This includes: ESD flooring and work surfaces with continuous monitoring, ionizers at critical process points (Solder Paste Printing, component placement), ESD smocks and gloves for operators, wrist straps with monitoring at assembly stations, humidity control to maintain appropriate relative humidity (typically 30–70% RH), and regular auditing and certification of the entire ESD control system.
For some medical device assemblies — particularly those involving implantable components or sterile field devices — additional environmental controls apply. Assembly may need to occur in ISO Class 7 or Class 8 cleanrooms with HEPA-filtered air supply, particulate monitoring, and personnel gowning protocols. The specific requirements depend on the device classification and the manufacturer's quality system.
Request their ESD control plan documentation, their most recent ESD audit results, and evidence of personnel ESD training. If your device requires cleanroom assembly, ask for the cleanroom certification documentation — ISO Class rating, last certification date, and particulate monitoring records.
ISO 13485 and FDA QSR require process validation for all manufacturing processes that can't be fully verified by subsequent inspection and testing. For Pcb Assembly, this means demonstrating — through documented evidence — that the assembly process consistently produces boards meeting their specifications.
The standard framework is IQ/OQ/PQ:
For medical device assembly, the PQ phase is the most important and the most commonly under-invested in. PQ isn't a one-time test run — it's a continuous demonstration that the validated process remains in control. This requires statistical process control (SPC) data: first-pass yield tracking, Solder Paste volume measurements, AOI defect rates, test yields, and process capability indices (Cpk) for critical parameters.
In Medical Device Manufacturing, traceability isn't a nice-to-have feature — it's a regulatory requirement and a patient safety imperative. When a field failure occurs, the ability to quickly identify which boards are affected, which manufacturing lots they're from, and what components went into them is the difference between a targeted recall and a blanket recall affecting your entire product history.
Medical device traceability for PCB assembly operates at multiple levels:
A Class II device fails in the field after 18 months of operation. Investigation reveals a solder joint voiding issue that caused intermittent connection failure under thermal cycling. With full lot traceability, you can identify the specific component lots, the boards from that manufacturing period, and issue a targeted recall for those serial numbers. Without traceability, you may be forced to recall every device ever shipped — a consequence that can cost tens of millions of dollars and destroy customer trust in your product line.
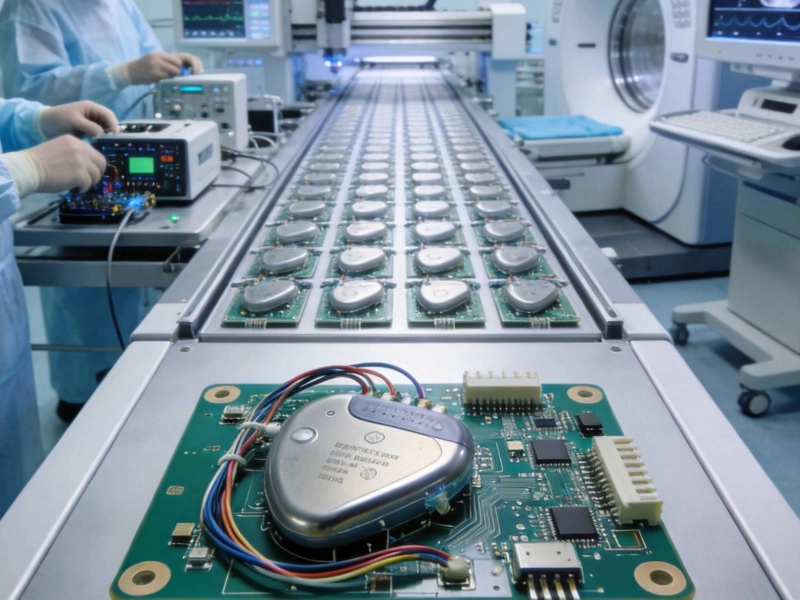
Standard production test — AOI, ICT, flying probe, functional test — is necessary but not sufficient for medical device assemblies. Medical device testing extends beyond verifying that the board functions correctly at the moment it ships, to demonstrating that the board will continue to function correctly over its intended service life and under the environmental conditions it will encounter in clinical use.
Environmental stress testing: Boards may be subjected to temperature cycling, thermal shock, humidity exposure, and vibration testing to verify solder joint reliability over the product's service life. This is especially critical for devices that will be sterilized (autoclave, EtO, gamma radiation) or implanted.
Accelerated life testing: Boards are operated under elevated stress conditions to accelerate failure modes that would take years to appear under normal use. The test data is used to project field reliability and service life.
X-ray and cross-section analysis: For boards with hidden joints (BGAs, QFNs), X-ray inspection is used to verify solder joint quality. Periodic cross-section analysis physically sectioning boards and examining the joint microstructure provides additional assurance of process quality.
Continuity and isolation testing: Beyond standard ICT, medical devices may require more extensive testing coverage — testing every net, every component value, and every isolation barrier to tighter tolerances than standard production test.
Functional test under clinical conditions: Where possible, boards are tested under conditions that simulate actual clinical use — with the clinical interface, the sensors, the actuators that the board will drive in the actual device. This catches interface issues that bench testing misses.
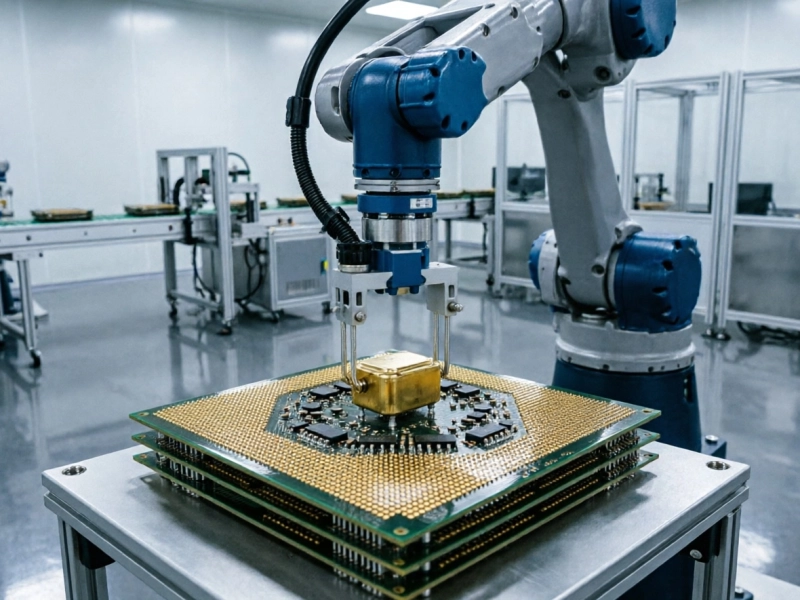
Implanted electronics — pacemakers, cochlear implants, neurostimulators, implantable monitors — face unique assembly challenges. Boards must be assembled with materials and processes compatible with implantation: no flux residues that could cause tissue reaction, biocompatible coatings where required, hermetic sealing verification, and sterilization process compatibility (EtO gas or gamma radiation sterilization). Assembly typically occurs in ISO Class 7 or cleaner cleanrooms, and the manufacturing process is often validated for 100% inspection coverage of critical parameters.
Devices that will be sterilized between uses — surgical instruments, endoscopy equipment, diagnostic equipment with patient contact — must withstand repeated sterilization cycles (autoclave, EtO, gamma, or chemical sterilization) without degradation of reliability. The PCB assembly process must be qualified against the specific sterilization method the device will use, including testing of board integrity, solder joint reliability, and coating/Conformal Coating durability through simulated sterilization cycles.
Choosing a manufacturing partner for Medical Device Pcb assembly is one of the most consequential decisions in your product development process. The qualification process should be thorough and rigorous — you're trusting them with patient safety as much as with your product quality.
"We spent six months qualifying our manufacturing partner for a Class II device. Three months of that was auditing their quality system in detail — and finding gaps that they then closed before we released production. That six-month investment has paid us back tenfold in the three years since. We've had exactly one field complaint, one CAPA investigation, and zero recalls. The upfront qualification work isn't optional. It's the foundation that everything else is built on."
— Director of Quality, Medical Device Company, Minneapolis
Medical Device Pcb assembly is demanding. The quality requirements are stringent, the documentation burden is real, the process validation is extensive, and the regulatory scrutiny is ongoing. None of this is news to anyone working in healthcare electronics — but it bears repeating, because the temptation to cut corners on manufacturing rigor is always present, and the consequences of doing so are always severe.
The companies that do this well — that have built manufacturing capabilities matched to the rigor of their devices — share a common characteristic: they treat manufacturing as an integral part of their product development and regulatory strategy, not as a service to be outsourced and forgotten. Their manufacturing partners are extensions of their quality systems, not black boxes that receive files and ship boards. The relationship is built on transparency, audit rights, shared responsibility for patient outcomes, and a recognition that every board that leaves the factory will eventually be in or on a patient.
That framing isn't comfortable for everyone in the supply chain. But it's the one that produces devices worthy of the trust that patients and clinicians place in them. When a surgeon reaches for a surgical robot, when a clinician adjusts an infusion pump dose, when a patient relies on an implanted device to regulate their heart rhythm — the chain of confidence that makes that moment possible includes every person who built, tested, and documented the PCBs inside that device.
High-reliability PCB assembly for medical devices demands more than ISO 13485 certification on paper. It demands engineering depth, process rigor, traceability systems, and a quality culture that takes every requirement seriously because patient safety is always on the line. Our team has built medical device electronics for Class I, II, and III devices across surgical robotics, diagnostic equipment, therapeutic devices, and implantable systems. Share your device requirements for a capability assessment and discover what medical-grade manufacturing looks like when it's done right.
ISO 13485 is the foundational Quality Management standard required for medical device manufacturing in most major markets. For PCB assembly specifically, it requires documented processes for every step that affects product quality, process validation, traceability systems, and a CAPA system. ISO 13485 certification is the baseline — but the depth of actual compliance, not just certificate status, is what matters. Ask for evidence of actual process validation, not just quality manuals.
Process validation proves that the manufacturing process consistently produces boards meeting specifications (IQ/OQ/PQ as described above). Product testing verifies that specific boards meet their performance requirements. Both are required, and they're complementary. You can have a well-validated process that produces a board that fails functional test due to a component issue. You can have passing functional test results from boards produced by an unvalidated process — which means you have no assurance the next board will pass. Medical device standards require both: validated processes and product testing.
It depends entirely on their actual quality system depth, not their marketing claims. Many standard EMS providers hold ISO 9001 and claim to support medical devices. ISO 9001 is not ISO 13485, and the requirements are materially different. Before committing, audit their quality system against ISO 13485 requirements, review their process validation documentation, verify their ESD and cleanroom capabilities if applicable, and check references from medical device customers in your device class. If they can't pass a rigorous qualification audit, they can't support your device.
The Device History Record (DHR) is the core document — it proves that a specific board was built according to the Device Master Record (DMR, which defines the product specifications) using the processes described in the Device Master Record. The DHR must include: component lot traceability (linking each component to its manufacturer lot), production records (which machines, operators, process parameters), inspection and test results, any nonconforming product records, and rework records if any rework was performed. For regulated devices, the DHR is subject to regulatory review during audits and inspections.
Counterfeit components are an industry-wide problem, and medical devices are particularly sensitive to the risk because field failures from counterfeit parts can harm patients and trigger regulatory action. Medical device EMS providers should source exclusively from franchised distribution or manufacturer-direct, maintain chain-of-custody documentation for all components, perform incoming inspection that includes visual verification and testing against datasheet specifications, and maintain records that support traceability back to the manufacturer. Ask your provider for their counterfeit component prevention policy and evidence of their sourcing controls before qualifying them for medical device work.
Why High-Reliability PCB Assembly is Critical for Medical DevicesJune/02/2026
How Automotive Electronics are Redefining PCBA Quality StandardsJuly/01/2026

The State of Global PCBA Manufacturing in 2026 and Key TakeawaysMay/22/2026
Understanding the True Cost Drivers in Modern Electronics ManufacturingJuly/20/2026
Navigating the Shift: Low-End vs. High-End PCB Assembly MarketsJune/12/2026

The Rise of AI Servers and Their Impact on HDI PCB AssemblyJuly/10/2026

How Turnkey Providers Streamline Component Procurement and LogisticsJune/18/2026

How We Handle Rush Orders and Quick-Turn PCB PrototypingJuly/08/2026